What are digestive tract polyps?
The development of a large part of the tumors of the digestive tract, especially colon cancer, the sequence of events that occurs involves the development of a precancerous lesion that in medicine is known as “adenoma” in its different forms, and which , popularly, are known as “Polyps”
Therefore, some “polyps” are premalignant lesions of the digestive tract.
What symptoms does it cause?
Usually these polyps rarely produce symptoms, except when they are located in the final section of the colon, very close to the anus, and grow enough that they can cause the appearance of blood mixed with feces.
How are they diagnosed?
The way to diagnose premalignant lesions of the digestive tract almost always involves invasive methods. However, when they are large enough and protrude into the lumen of the colon, they can also be seen in imaging tests. Knowing, in addition, that sometimes these lesions produce minimal bleeding, undetectable when the feces are examined with the naked eye, a Fecal Occult Blood test can be performed (necessarily with three samples of three different stools and preferably using a test that is called immunological), to detect the presence of blood not detected visu.
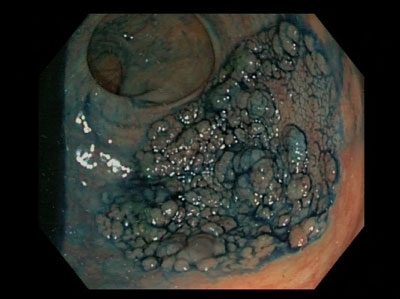
Despite everything, the most precise tests that detect the most lesions are endoscopies: Gastroscopy for lesions of the esophagus, stomach and duodenum, Colonoscopy for lesions of the colon and rectum and capsule endoscopy / enteroscopy for lesions of the small intestine.
How are they treated?
If within medicine there is controversy when it comes to addressing different problems, in the case of colon polyps there is a great consensus to always treat them endoscopically, regardless of size or location, it seems reasonable to assume that the first option should always be If the option is to remove these lesions by endoscopy, since it avoids unnecessary surgery for the patient, recovery is always quick and in no case does it involve mutilation of the patient.
An attempt should be made, as far as possible, to remove these lesions in a single piece, which is always sent to the specialist in Pathological Anatomy, our expert in looking at the lesions under the light of the microscope, and who is the one who tells us, after the thorough examination of the piece, that the polyp is completely removed and the “name and surname” of the polyp, which always has a fundamental value when considering endoscopic surveillance of the patient.
To remove these polyps completely and in one piece, we have several endoscopic strategies.
SIMPLE POLYPECTOMY
Simple polypectomies, which are performed with a polypectomy snare, are routinely performed in any endoscopy suite. It consists of linking the polyp with a instrument, called a “diathermy handle” and, applying electric current or without it, in the case of lesions smaller than a centimeter, completely sectioning the polyp.
SUBMUCOSAL ENDOSCOPIC DISSECTION (ESD)
DSE is the endoscopic technique through which we remove large lesions, both from the colon, the stomach and sometimes in the small intestine.
These types of lesions, known as Lateral Spreading Tumors (LST), have a greater risk of having crossed the adenoma threshold (premalignant lesion), to have entered the path of adenocarcinoma (cancer). For this reason, it is essential that the piece be removed in a single block, because in the event that progression towards colon cancer has occurred, the Pathologist can tell us exactly at what point in the lesion the transformation has occurred, identifying how much healthy tissue there is around it, to know if the patient is cured or not.
In order to completely remove the lesion and do it in one piece, the DSE technique was developed in Japan and later exported.
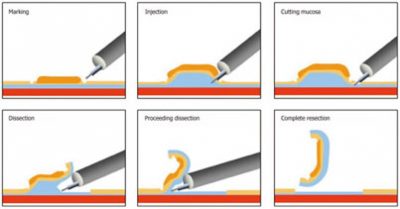
Endoscopic dissection is a demanding technique, which is carried out in a few hospitals in the national territory and consists, literally, of removing the most superficial layer of the digestive tube from the rest of its layers, in order to isolate the injury to the rest of the digestive tract. In this way we are able to remove lesions regardless of their size, the only limit is the experience of the endoscopist.
In the Advanced Endoscopy Unit of the QuirónSalud Hospital in Málaga, we have the human, technical and technological methods necessary to carry out both simple polypectomies and the more complex and advanced submucosal dissection techniques, both in the stomach and colon, as well as actively participate in the dissemination of the technique to the rest of the hospitals, at the national level, organizing sessions and courses periodically and frequently with international speakers of highly recognized prestige worldwide. We are a reference unit in DSE throughout the national territory and the center with the most experience in this technique south of Madrid.